A 50 yr Old male with abdominal distension
A 50 year old male with abdominal distention
This is an a online e log book to discuss our patient de-identified health data shared after taking his / her / guardians signed informed consent. Here we discuss our individual patients problems through series of inputs from available global online community of experts with an aim to solve those patients clinical problem with collective current best evident based input.
This E blog also reflects my patient centered online learning portfolio and your valuable inputs on the comment box is welcome.
I have been given this case to solve in an attempt to understand the topic of " patient clinical data analysis" to develop my competency in reading and comprehending clinical data including history, clinical findings, investigations and come up with diagnosis and treatment plan
The patient/ attender was informed the purpose of the information being acquired. An informed consent was taken from patient/ attender and there is omission of information that was requested to be omitted.
CONSENT WAS TAKEN FROM BOTH PATIENT AND ATTENDERS
Chief complaints :
A 50 year old male came with complaints of
-Abdominal distention and pain abdomen since 8 days
-Shortness of breath since 8 days
-Bilateral lower limb swelling since 6 days
-Decreased urine output and yellowish discoloration of urine since 6 days
HISTORY OF PRESENTING ILLNESS:
-Patient was apparently asymptomatic 8 days back
then he had abdominal distention which was diffuse associated with abdominal pain which is squeezing type ; aggravated with food intake .
-Complaints of bilateral pedal edema which is pitting type extending from ankle to knee joint since 6 days.
-He had decreased urine output and yellowish discolouration of urine since 6 days
-Not associated with fever with chills and burning miturition .
-Complaints of shortness of breath with grade II which is decreased in supine position
-No H/o hematemisis , melena
PAST HISTORY:
-No similar complaints in the past.
-3 years back he was admitted in hospital for 15 days and was diagnosed with dengue .
-2 years back he had jaundice for which he had a 2 PRBC transfusions
-Recently 20 days back he is having decreased vision so he went to checkup and diagnoses with cataract , he was adviced to stop alcohol so he stopped alcohol 15 days back
Not a known case of HTN , Diabetes , asthma , TB , epilepsy , CAD , thyroid diseases
Personal history
He is a government revenue employee who wakes up at 6 am ;do his daily routine and goes to his work . Most of the time he skips his breakfast and has lunch at around 2 pm to 3 pm and comes to home at around
6 pm then he goes to drink alcohol-whiskey 180 ml this was his daily routine since 12 years .
He takes mixed diet
-Appetite : decreased since 6 days
-Sleep : adequate
-Bowel : regular
-Bladder :decreased urine output since 6 days
-Addictions :Alcoholic since 12 years,he used drink 180 ml of whiskey twice a week but from last 6 years he began drinking 180 ml of whiskey daily, but stopped drinking 15 days ago.
- No h/o smoking
Family history
No history of similar complaints in any of his family members
GENERAL EXAMINATION
Patient was conscious,coherent and cooperative. Moderately built and nourished
-Pallor : present
-Icterus: absent
-Clubbing: absent
-Cyanosis: absent
-Lymphadenopathy: absent
-Edema : present









VITALS:
On 2/1/23
Temp : afebrile
BP : 110/90 mmHg
Pulse : 90 bpm
RR : 22cpm
Spo2 : 98%
On 3/1/23
Temp: afebrile
BP : 110/70 mmHg supine position
Pulse : 92 bpm
RR : 20cpm
Grbs : 101 mg /dl
On 4/1/23
Temp: afebrile
BP: 110/70 mm Hg
Pulse: 82bpm
RR:18cpm
SYSTEMIC EXAMINATION
PER ABDOMEN
INSPECTION:
-Abdomen is distended
-dilated veins are seen
-Flanks are full
-Umbilicus : flat
PALPATION:
-No local rise of temperature
-Abdomen is tense
-Abdominal girth : 92 cms
-Mild tenderness over right hypochondrium
-Liver and spleen are not palpable.
- Shifting dullness present
- Fluid thrill absent
PERCUSSION:
-A dull note is heard
ASCULTATION:
-bowel sounds not heard clearly

 Left side of abdomen
Left side of abdomen

RESPIRATORY SYSTEM:
INSPECTION:
- Trachea Is central
-Shape of chest is normal
-Expansion of chest is equal of both sides
-No scars and sinuses
PALPATION:
-no local rise of temperature and tenderness
-All inspectory findings are confirmed
PERCUSSION:
- resonant note heard
ASCULTATION:
-Normal vesicular breath sounds heard
CVS :
-S1 S 2 heard apex beat felt at 5th inter coastal space lateral to mid clavicular line
-No murmors
CNS examination
HIGHER MENTAL FUNCTIONS:
Conscious, coherent, cooperative
Appearence and behaviour:
Emotionally stable
Recent,immediate, remote memory intact
Speech: comprehension normal, fluency normal
CRANIAL NERVE:
All cranial nerves functions intact
SENSORY FUNCTIONS
SPINOTHALAMIC TRACT
Pain , temperature ,presure- intact in all limbs
Posterior column:
Fine touch, vibration and proprioception are intact
MOTOR SYSTEM :
Right Left
Bulk:
Inspection. N. N
Palpation. N. N
Tone:
UL. N. N
LL. N. N
REFLEXES :
B T S K A P
R + + + + + Flexor
L + + + + + Flexor
CEREBELLUM:
Finger nose Incoordination - No
Knee heel incoordination - No
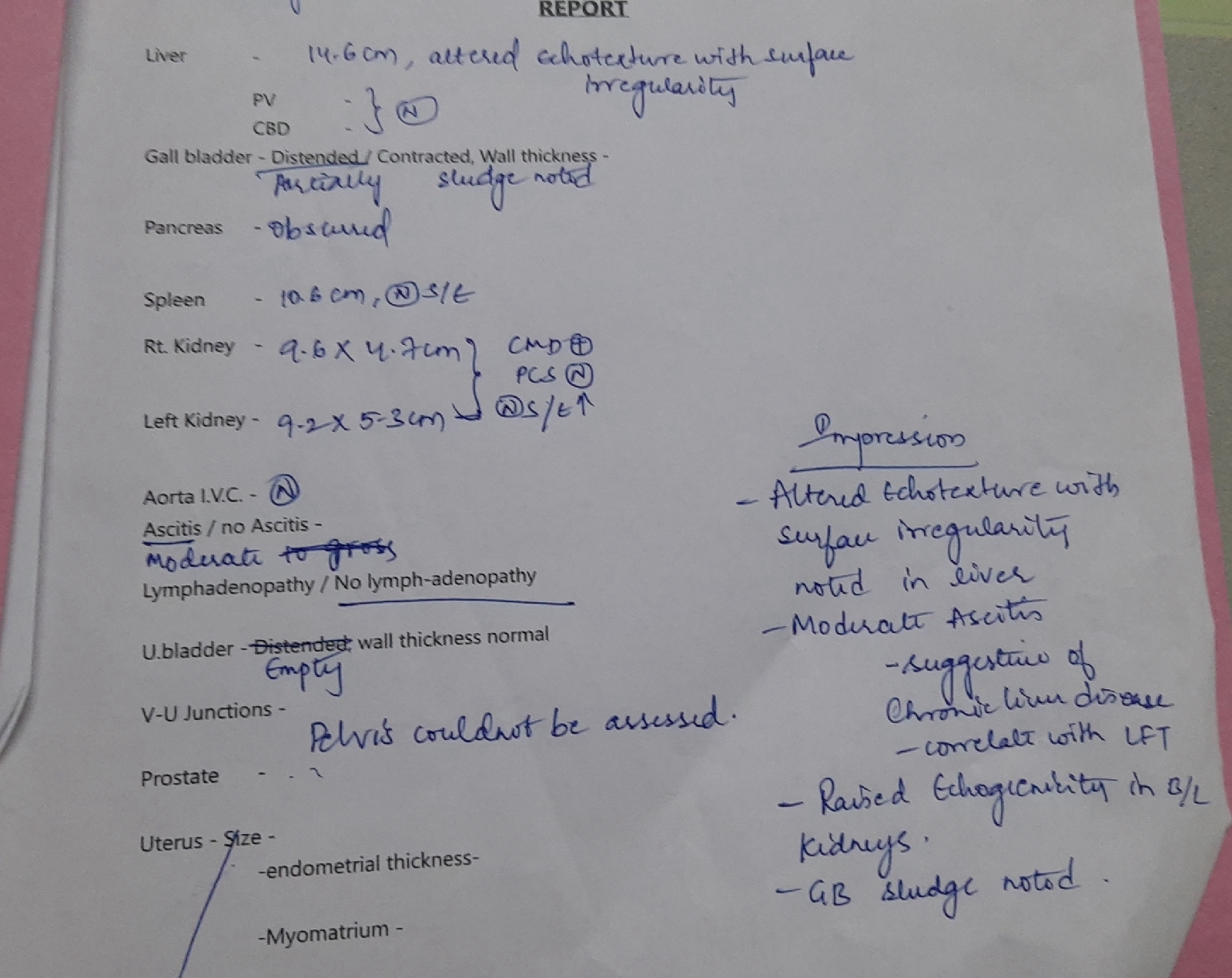
DIAGNOSIS
Decompensated liver disease and pancreatitis secondary to alcohol intake.
INVESTIGATIONS









TREATMENT :
Ascitic tap was done but no fluid was drained
• Fluid restriction less than 1.5 L /day
• Salt restriction less than 2g/day
• Inj Lasix 40mg IV BD
• Syp lactulose 30ml PO
• Inj Monocef
• TAB Aldactone 50 mg PO OD


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Comments
Post a Comment